News
The importance of properly diagnosing distal radius fractures
26 April 2021
Most of us know it as a broken wrist, but the medical term is a distal radius fracture. Most interesting is that the bones of the wrist, the carpal bones, are not generally where the break is, but usually about one inch from the distal end (toward the wrist) of the radius bone (the larger of the two arm bones).

These types of fractures are generally caused by a fall on outstretched hands but can also occur during various sporting activities. In people older than 60 years old, especially those with osteoporosis, distal radius fractures commonly occur due to a fall from a standing position.1 “Fractures of the distal end of the radius are common injuries, comprising 12% to 17% of all fractures.”2
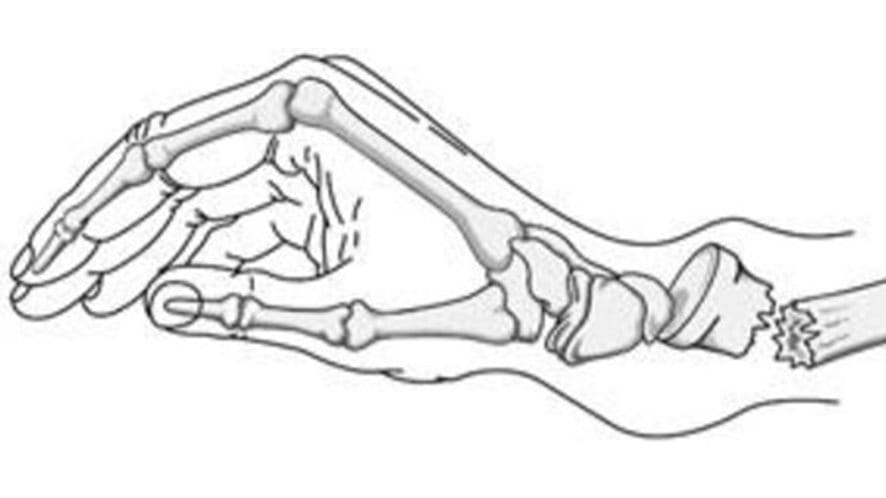
One of the most frequent types of distal radius fracture was first explained in 1814 by an Irish surgeon named Abraham Colles. In this type of “Colles’” fracture, the broken end of the radius bone tilts up, as depicted in this picture:1
According to the American Academy of Orthopedic Surgeons, “it is important to classify the type of fracture, because some fractures are more difficult to treat than others. Other ways the distal radius can break include:
- Intra-articular fracture. A fracture that extends into the wrist joint. ("Articular" means "joint.")
- Extra-articular fracture. A fracture that does not extend into the joint is called an extra-articular fracture.
- Open fracture. When a fractured bone breaks the skin, it is called an open fracture. These types of fractures require immediate medical attention because of the risk for infection.
- Comminuted fracture. When a bone is broken into more than two pieces, it is called a comminuted fracture.”1
Most people know there is something wrong with their wrist after a fall because they will experience instantaneous pain, tenderness, bruising and swelling, as well as noting their wrist is positioned strangely in a bent position. They may also feel numbness in their hand or a change of color in their fingers. Once examined, the doctor will order X-rays to show how badly the bone is broken and to determine which kind of treatment will be most effective. As with any break, the bones must be re-aligned and stabilized so that they can heal. With a simple break, this can be done without surgery, but in more extreme cases, surgery may be required to set the bone for healing. 1
While “the conservative treatment of closed reduction and casting has historically been the mainstay of treatment”3, the risks of poor long-term outcomes must be considered. The main complications seen include the following:
- Malunion: This is the most common complication that occurs after a distal radius fracture. This happens when the fracture heals without the proper alignment of the bones, the joint, or incorrect length of the bones. This type of complication can be seen in “35% of patients treated conservatively.”3
- Complex Regional Pain Syndrome: Pain that affects the function of the wrist as well as the of skin and muscles of the wrist area; can be seen in conservative treatments where there is increased pressure under the cast, sometimes involving the nerves.
- Infection: Mostly after surgical repair, infections can be seen in up to 33% of patients.3
- Tendon complications: Seen after surgical repair, the tendon can form adhesions, lacerate or rupture, usually occurring around 7 weeks after repair.3
Malunion complications might be prevented with proper diagnosis and treatment. Poor diagnosis coupled with the lack of training or experience in properly reducing the fracture may lead to the need for surgical correction, “a challenging problem with unpredictable outcomes. Prevention of malunion of a distal radius fracture is the best course of action”.2

Limbs & Things is proud to present a new product focused on the conservative treatment for Colles’ fracture. Designed in collaboration with Dr Salwa Malik of Brighton and Sussex University Hospitals NHS Trust and Dr Yasir M. Shaukat of Surrey and Sussex Hospitals NHS Trust, the Colles’ Fracture Reduction Trainer provides trainees with a platform for repeatable and consistent practice of manual Colles’ reduction (closed) and plastering techniques.
Based in the United Kingdom, Dr Shaukat and Dr Malik identified the requirement for a training solution that facilitates the resetting of fractures at the distal end of the radius and also takes into account the pain and uncomfortable nature associated with the procedure. As is typical in a real-life emergency setting, the model allows trainees to perform visual inspection and identification before facilitating a team focused Colles’ fracture reduction. For advanced learning, an adjustable tension mechanism harnesses the ability to simulate more difficult procedures where the bones are more difficult to reset and align.
Contact our team to find out more.
References:
1: American Academy of Orthopedic Surgeons: Distal Radius
2: Distal Radius Malunion
3: Management of Complications of Distal Radius Fractures